Abstract
This paper is a technology report determining the market feasibility of a spine surgical navigation system, X23D, a computer system whose AI creates a 3D model of the patient's spine. Paired with a third-party instrument-tracking system, the two devices help the surgeon place screws in the patient's lumbar spine. The scientific discussion reveals that X23D has a competitive advantage due to its unique AI training, 3D modeling, and instrument tracking. However, an ex-vivo study reveals that X23D produces a higher clinically significant breach rate in lumbar fusion than its 2D and 3D competitors, a statistic that seemingly eliminates its feasibility. A SWOT analysis shows this breach rate is the only weakness limiting absolute feasibility; a PESTLE analysis shows external factors that lessen the outward concern, giving a green light for a Blue Ocean strategy. That strategy identifies X23D's best customers as very experienced surgeons who are unaware of X23D's 3D competitors and who care about lowering cost and radiation. Because a valid customer base exists, and because a substantially equivalent device (Zeta Surgical) makes a trial possible, X23D has limited feasibility that depends on a specific marketing plan. Once the AI matures and clinically significant breaches fall, X23D could become the best navigation system in the market.
Introduction
The Medtronic Stealth surgical navigation system was set to revolutionize the surgical realm. However, two catastrophes hit the product. First, patient deaths occurred because surgeons used unapproved devices with the system (Jackson, 2017). Second, massive Class 1 FDA recalls of Medtronic Stealth systems (CDER, 2023), unrelated to the unapproved devices, sent the system back to the drawing board.
The takeaways: the patient deaths reveal that the customer's needs and environment were not taken into account during the selling process; had they been, doctors would not have reached for unapproved devices. The recalls reveal that the underlying science was not sound and that proper clinical trials were not done. What could have prevented both? A proper technology feasibility review, one containing a rigorous scientific discussion, an evidence-based clinical trial, a marketing plan, and strategic analysis of customer need and external factors. To demonstrate how such a report is done, a revolutionary spine surgical navigation system, X23D, is taken as the example throughout this discussion.
Brief introduction of X23D
X23D is an imaging medium in which an AI computer system constructs a 3D model of the spine intra-operatively using a few X-ray images taken right before the operation. It does not have its own instrument-tracking system, but it can be paired with one. The system has been proven to complete lumbar pedicle-screw insertion only. Commercially, the technology was built as a project within a university research group; it has done no human clinical trials and is not being sold.
Scientific background and discussion
Artificial-intelligence background of X23D
AI is a computer system that can learn and make decisions somewhat like a human. Instead of just following commands, it learns and reasons from large amounts of data, finds patterns, and applies those patterns to data it has not seen before. (Feed an AI 10,000 photos of cats and dogs and tell it what makes them different; afterward it can guess whether a new photo is a cat or a dog.)
X23D's AI works through a method called transfer learning. Before transfer learning, CT scans of different spines are taken from a public database and the 3D structure of a spine is generated. From this 3D model, thousands of artificial X-ray images are produced from every possible angle, clean images without real-world blemishes such as noise, poor image quality, or anatomical variation. These are the initial training dataset. Transfer learning then feeds the AI both the pristine images and real-world blemished X-rays, teaching it to trace the spinal landmarks from the perfect images onto the same landmarks in blemished ones. Fed a new blemished spine image, the AI finds those landmarks and builds a 3D model, in effect reversing the process that created its initial training set.
Why does this matter? Competing navigation systems must take multiple 2D images (CTs, X-rays) to produce a 3D image, and their cleanup AI is trained on radiology scans of real patients, the only images the trainers can acquire. That demand for real clinical data requires more scans, increasing patient radiation exposure and cost. X23D, by contrast, generates its own training X-rays and can even alter them for training.
Why not use CT images instead of X-rays to build the spine? CT takes surrounding tissue into account, but X23D's current procedure, pedicle-screw insertion in the lumbar region, relies on cortical bone landmarks only, so tissue awareness is not needed. Using CT would also erase X23D's competitive advantages of lower radiation exposure and cost.
Surgical-navigation background of X23D
Spine surgical navigation refers to any system that guides the surgeon through a procedure by visually noting instruments and implants in real time over an imaging medium. Imaging mediums include CTs, X-rays, and artificially created models, in either 2D or 3D, with or without an instrument-tracking system.
Figures reproduced from the original report. Tables 1–2 below compare imaging mediums (2D vs. 3D) across X-ray, CT, and reconstructed-model modalities. The clinical figures are third-party images, each cited beneath the figure and in the References.
| 2D | 3D | |
|---|---|---|
| X-ray |

Figure 1: 2D X-ray, no instrument tracking Cage implant visible on the superior cervical vertebra (bright white). From Figure 2-5 [Image], drzezzo, 2019, Musculoskeletal Key. |
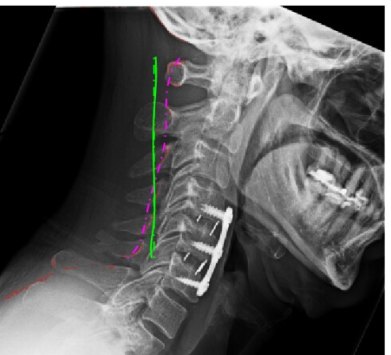
Figure 2a: 3D X-ray, no implant tracking Implants (bright, triangular) shown digitally in the upper cervical spine. From Figure 4(c) [Image], Eniko & Rein, 2014, JME. |
| CT scan |

Figure 3: 2D CT, no instrument tracking Spine implant indicated by the arrow. From Fig 8 [Image], Hayashi et al., 2012, AJR. |
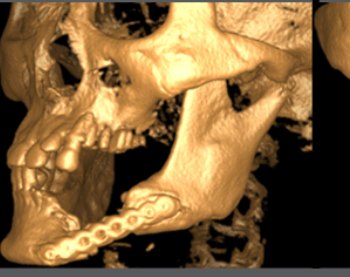
Figure 4: 3D CT, no instrument tracking 3D CT of cervical spine and jaw; illustrates how surgeons view implant position. From Cover Figure [Image], IJCRI, 2016, Edorium Journals. |
| Reconstructed model | N/A |
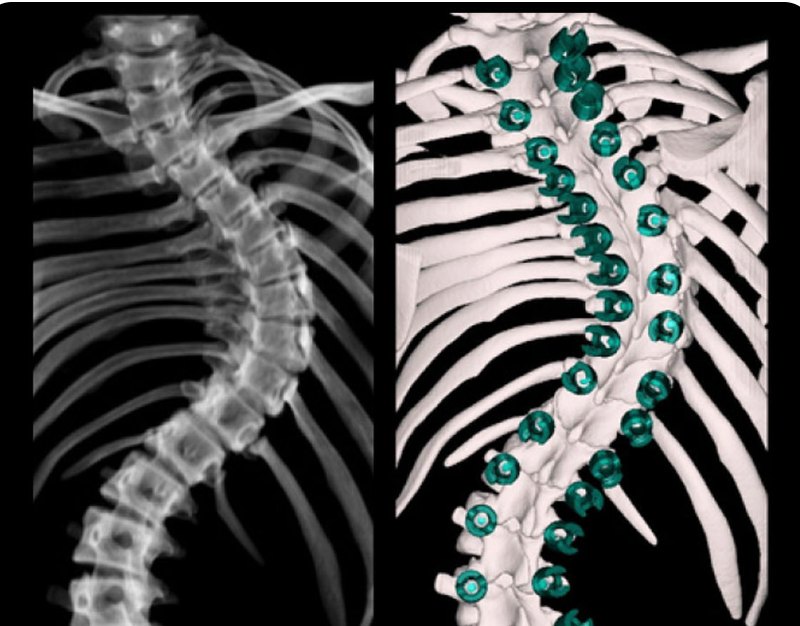
Figure 7: 3D model, no instrument tracking 3D model of spine vertebrae on screen during patient registration. From Software Features [Image], CBYON Eclipse, 2024, MSS. |
Note. Reconstructed digital models of the spine are typically 3D, so the 2D cell is empty. All figures are individually cited in the References.
| 2D | 3D | |
|---|---|---|
| X-ray |

Figure 5: 2D X-ray with instrument tracking Blue instrument represents the real-time location of the tool on the spine. From SpineMap Go [Image], Stryker NAV3i Platform, 2025. |
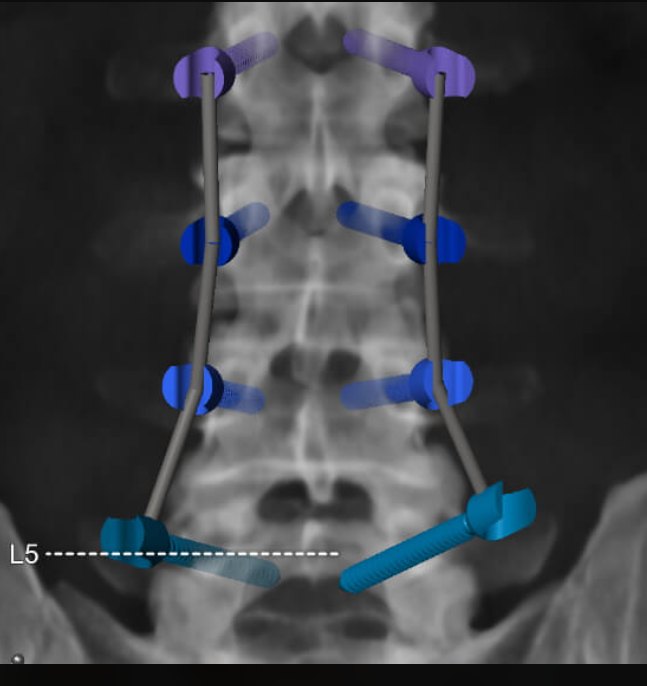
Figure 6a: 3D X-ray with implant tracking Implants (blue and purple) shown digitally, real-time, in the lumbar spine. From Spinal Planning [Image], BrainLab, 2025. |
| CT scan |
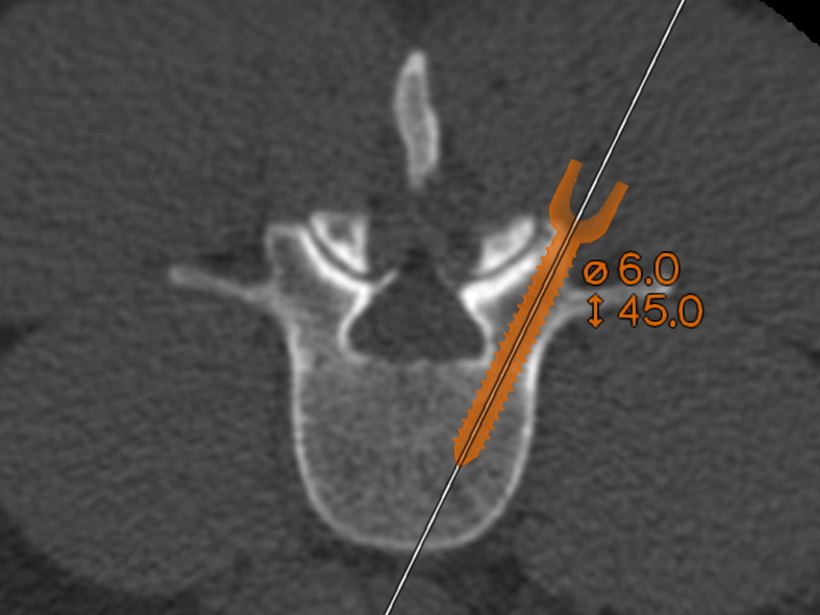
Figure 7: 2D CT with instrument tracking Orange implant marks the current location of the screw being placed. From How Spine Navigation Amplifies Surgery [Image], BrainLab, 2025. |
Figure 8: 3D CT with instrument tracking Blue instrument and green trajectory show real-time location and path. From Fig 4 [Image], AO, 2023, AO Foundation. |
| Reconstructed model | N/A |

Figure 6: X23D's 3D model with paired instrument tracking X23D's 3D model of vertebrae (red) on screen; the yellow instrument shows current location and trajectory (blue). From Fig 2 [Photograph], Luchmann et al., 2024, BMC Musculoskeletal Disorders. |
Note. Instrument tracking displays digital implants/instruments and their trajectory over the imaging medium. Figure 6 is X23D's own system. All figures are individually cited in the References.
Imaging dimension. 3D models give better instrument precision and implant placement (e.g., instrument height is visible in a 3D CT but not a 2D CT). 2D imaging requires many shooting sessions from multiple angles. Both 2D and 3D require images before and during surgery, increasing radiation and case time (and therefore cost). Because X23D produces a 3D model, its instrument precision and implant placement should exceed 2D navigation; because it needs only four intra-operative X-rays right before incision, radiation and procedure cost should fall for both patient and surgical team.
Instrument tracking. Real-time tracking improves implant placement (DeVito et al., 2010) but its disadvantage is patient registration, the surgeon telling the system where the spine is relative to the imaging medium. If the patient shifts, registration restarts. Without tracking, the system must repeatedly image the site and instruments, lengthening the case (especially with X-rays). X23D integrates tracking into its 3D imaging, and, crucially, automates registration: the operating bed carries a titanium-bead calibration module that acts as the frame of reference for both the 3D model and the tracking system, so image capture and registration happen at once. This saves time and lowers radiation for everyone.
X23D workflow, start to finish
X23D operates intra-operatively in the OR. The patient lies on the table with a calibration device containing titanium beads, which acts as the frame of reference between the on-screen 3D model / instruments and the physical position of the spine. Four X-ray images are taken from four views and fed into the X23D computer, where an advanced algorithm builds a 3D model of the lumbar spine, about 81 milliseconds per vertebra, using spatial information from the bead module. No additional patient registration is needed because a third-party optical tracking system also uses those beads for spatial referencing. Surgeons then see the position of the 3D model and instruments on the overhead display, and pedicle-screw insertion begins.
Key definitions
The study procedure is a pedicle-screw insertion ("lumbar fusion"). The surgeon places pedicle screws into the pedicles of vertebrae that were already fused with bone graft; screws in adjacent vertebrae are then connected vertically with a rod. The main errors are breaches, when a screw deviates left or right from the center of the pedicle and breaks the pedicle wall, threatening vital structures. More deviation means a more severe grade. A clinically significant breach is Grade 2 or higher, a deviation of 2 mm or more.
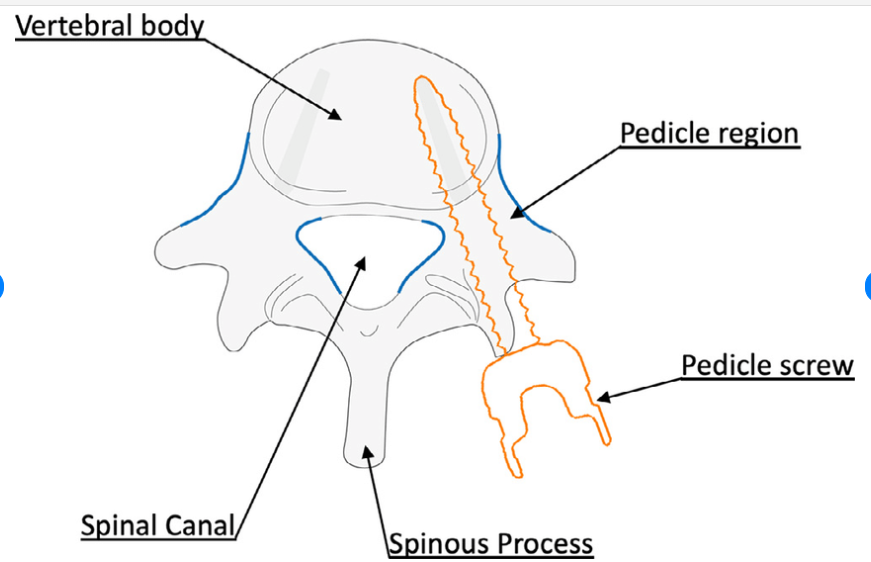
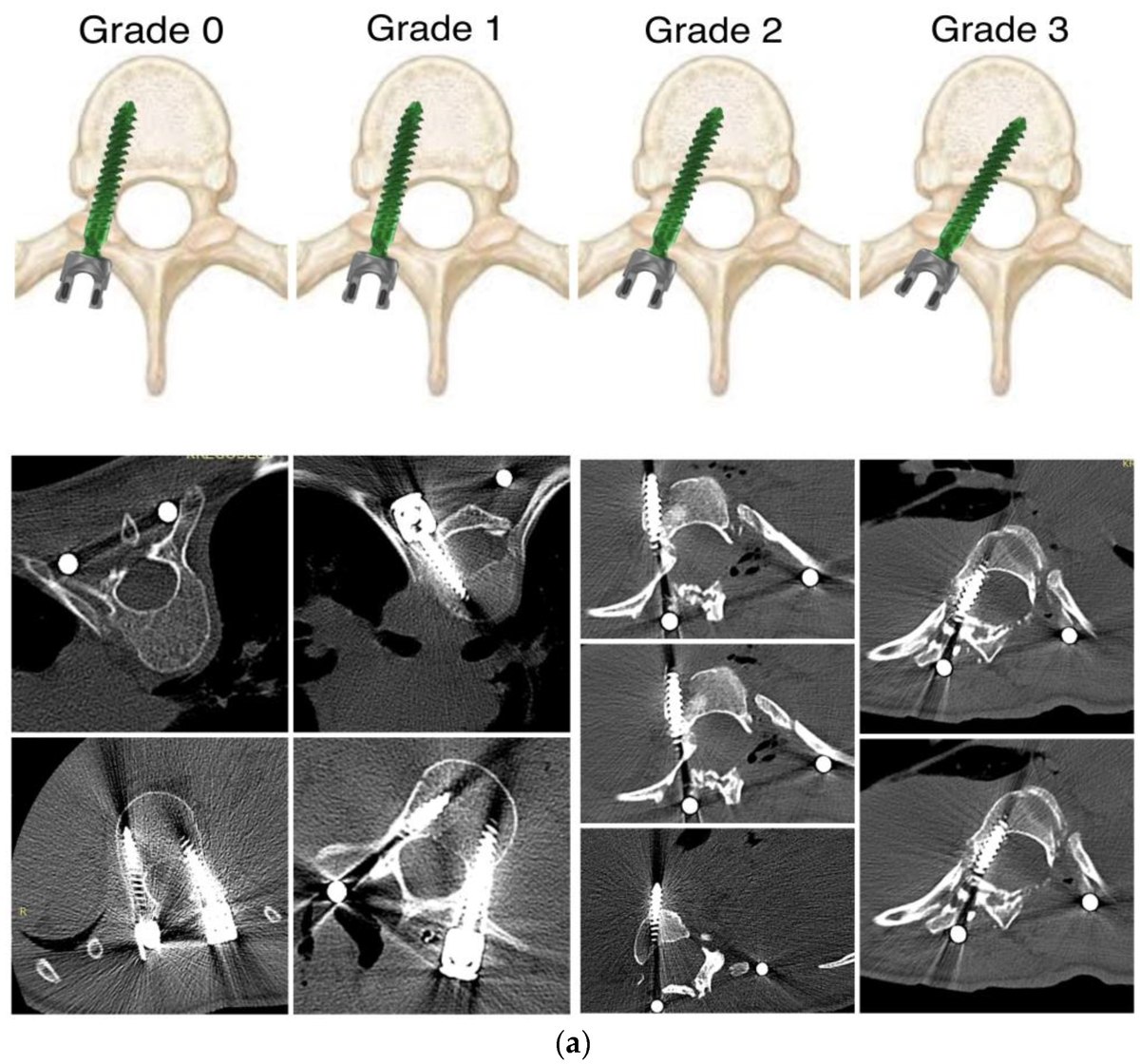
Table 3: Pedicle-screw insertion vs. breach. The figures show unilateral insertion; the same breach rules apply to bilateral insertion. All figures are cited in the References.
Surgical results of X23D
The scientific proof comes from an ex-vivo study in which surgeons inserted pedicle screws into the lumbar spines of cadavers in two groups: one using X23D plus a paired instrument-tracking system, the other using traditional 2D X-ray navigation. The most significant results, overall breach rate, clinically significant breach rate, and radiation exposure, are compared below against published 3D-navigation competitor data.
| System | Overall breach rate (%) | Clinically significant breach rate (%) | Radiation exposure (mSv) |
|---|---|---|---|
| X23D group, lumbar fusion | 21.00 | 12.00 | 9.98 |
| 2D X-ray control group, lumbar fusion | 24.00 | 8.00 | 14.84 |
| 3D-based navigation with instrument tracking | 25.60 | 6.20 | 18.30 – 30.00 |
Note. "mSv" = millisievert (higher = more radiation). X23D and 2D control data from Luchmann et al. (2022/2024). 3D-navigation breach data from Asada et al. (2024); 3D radiation data from Baumgart et al. (2023). Overall breach rate = screws deviating from the pedicle midline ÷ screws placed; clinically significant breach rate = Grade 2+ breaches ÷ screws placed.
The takeaway. X23D fulfills two of the customer's advantages, lowest overall breach rate and lowest radiation exposure. The one result that undermines feasibility is its highest clinically significant breach rate (12.00%). Overall breach rate matters less because Grade 0–1 breaches are often asymptomatic, whereas a Grade 2 breach can paralyze the patient. Telling a surgeon that X23D's major-breach rate is ~50% higher than competitors will not go well, but X23D cannot be solely blamed for those breaches, and the strategic plans below reduce the threat this poses to feasibility.
Strategic plans
SWOT analysis
Outside the defect of clinically significant breaches, X23D is broadly feasible. Lower radiation aligns with the WHO's push toward less radiation exposure, and the AI medical-imaging market's high CAGR (34.8%) means the market X23D enters is ripe for profit. The one strict threat to feasibility is the clinically significant breach rate; no other weakness or threat is a hard stop to release.
Strengths
- Less expensive and time-consuming than other 3D spine systems
- Lower overall error rate than other 3D spine systems
- Less ionizing radiation than other 3D spine systems
- Better user experience than traditional X-ray-guided spine surgery
Weaknesses
- Higher clinically significant breach rate than traditional X-ray-guided and other 3D navigation
- Limited to the lumbar area and lumbar pedicle-screw placement
- Lack of dedicated research and no completed human clinical trials
Opportunities
- CAGR of the AI-imaging market, 34.8%
- Healthcare movement to decrease radiation exposure
- Lumbar-fusion surgery rate expected to rise
Threats
- Evolving AI regulation nationally and internationally (EU AI Act, recent FDA legislation)
Table 5: SWOT analysis of X23D technology. Strength/weakness framing after Luchmann et al. (2022); market/regulatory data per Grand View Research (2023), WHO (2024), Lopez et al. (2020), EU Public Health (2025), and FDA (2025).
PESTLE analysis
A PESTLE analysis shows how external factors decrease the perceived severity of clinically significant breaches. For example, augmented-reality (AR) guided surgery and an upcoming X23D partnership both may decrease breaches (Chong et al., 2020); they are not listed as strengths because there is no evidence yet that they lower X23D's breach rate specifically, but they soften the initial reaction to it. Likewise, a higher major-breach rate looks less alarming while AI is not currently held legally liable for its mistakes, and while breaches can be attributed to over-reliance on navigation rather than the device alone.
- Political
- Although the FDA has approved many AI-based imaging devices, important regulatory gaps still persist.
- Economic
- X23D targets minimally invasive surgery, which tends to reduce complications and generate cost savings for health systems. Separately, some spine surgeons report patients paying for back surgeries they do not need.
- Sociological
- Substantial regional differences exist in US spine-surgery rates; patients with public or no insurance often face barriers to specialized spine care.
- Technological
- X23D requires intra-operative radiation, whereas some machine-vision systems (e.g., 7D navigation) use visible light and cameras, removing that need. AR headsets project virtual images onto the surgical field for greater accuracy.
- Legal
- Spine surgery faces a notably high incidence of malpractice litigation. The legal status of AI in medicine is evolving, with current trends denying legal personality to AI systems.
- Environmental
- Training AI models can emit hundreds of thousands of pounds of CO₂, and AI growth drives demand for energy-hungry data centers with advanced cooling.
Table 6: PESTLE analysis of X23D technology. Sources per the References below (Muralidharan et al. 2024; Taghva 2025; Clark 2024; Raad et al. 2019; Segal et al. 2018; Orthofix 2025; Chiou et al. 2023; Medress et al. 2020; Jassar et al. 2022; Hao 2020; Deloitte 2024).
Blue Ocean strategy
Rather than competing head-to-head with established robotic or CT-based systems, X23D expands the market by turning non-users of advanced navigation into adopters. Surgeons who prioritize patient safety will pick the competitor with the lowest clinically significant breach rate, so X23D must instead find surgeons unfamiliar with 3D navigation who know only 2D image-guided navigation, and emphasize its radiation and cost advantages over 2D. These surgeons are in more rural areas (not academic centers exposed to competitor devices) and tend to be older: more free-hand experience offsets the major-breach rate (experienced surgeons breach less, Samdani et al., 2010), and X23D's strong user experience eases adoption.
- Market focus
- Poorer, rural areas worldwide where 3D navigation is not well known and 2D fluoroscopy is standard, rather than wealthy academic centers.
- Value proposition
- Combines cost efficiency with advanced imaging; suits older rural surgeons who need a good user experience; adds little time versus traditional 2D-guided fluoroscopy.
- Customer segments
- Transforms non-users into navigation adopters, expanding the overall market.
- Eliminate / reduce
- Removes costly preoperative scans and large robotic systems.
- Raise
- Minimizes radiation exposure; enhances overall breach avoidance, workflow speed, and accessibility.
- Sustainable advantage
- Harnesses ongoing AI advancement and network-driven learning to build a "plug-and-play" brand that late entrants struggle to replicate.
Table 7: Blue Ocean strategy of X23D technology. Market-focus rationale after Lewandrowski et al. (2020).
Marketing plan
Positioning follows the Blue Ocean customer segment: rural, lower-income areas, emphasizing radiation safety and cost efficiency. Both points have support, Dr. Theodore Wagner argues hospitals should set strict radiation-exposure limits for surgeons (2021), and with "unnecessary spine surgeries" in the news (Clark, 2024), surgeons do not want to overspend, especially when charging low-income populations.
- Patients (billboards & flyers). Positioned near oncology centers and free health clinics; for low-income elderly near major oncology centers, the message emphasizes reducing cancer risk and cutting costs.
- Rural surgeons (clinic flyers). Delivered to surgeons' clinics and the ORs where they hold privileges, emphasizing less imaging, lower radiation, and shorter operating time.
- Insurers (LinkedIn & conferences). A limited initial push, kept small to avoid scaring insurers off with the higher major-breach rate, emphasizing smoother workflows and lower claims/reimbursement costs.
Clinical trial of X23D
X23D would pursue a process combining elements of a 510(k) clearance, enabled by a substantially equivalent device from Zeta Surgical, with characteristics of a Premarket Approval (PMA), reflecting evolving AI/ML device regulation under the FDA's 2024 AI/ML action plan. Because X23D's algorithm is more advanced than Zeta's, more clinical information would be needed for comparison.
- Preclinical validation (15–18 months, $3–4M). Tests 3D-model accuracy under adverse conditions (noise, poor positioning) and audits bias, using 5,000 annotated X-ray sequences across patient subgroups (BMI, age) so models are accurate across diverse populations.
- Pilot study (7–9 months, $2.5M). 20–30 patients with varied spinal shapes and deformities; goals: clinically significant breach rate below 7%, overall breach rate below 21%, radiation no higher than 10 mSv, with continuous algorithm monitoring.
- Pivotal clinical trial (20–24 months, $10–12M). Controlled, randomized, large-scale; 160–310 spinal-fusion patients randomized to X23D or CBCT-based navigation. Primary endpoint: pedicle-screw accuracy at least equal to CBCT (margin within 10%). Secondary: radiation (kept at 50% of other 3D systems), screw-insertion time (less than CBCT), and workflow interruptions; plus a learning-curve analysis.
- FDA review (6–12 months, ~$750K). Total program ≈ $17.2 million.
Because the trial tests an AI algorithm, extra controls apply: the algorithm must be frozen before the trial for data consistency; a Pre-Specified Change Control Plan must govern future modifications; and post-launch safety/accuracy monitoring (including cybersecurity for HIPAA) is required. Post-market, X23D would issue quarterly performance reports for the first two years and maintain a minimum five-year follow-up on radiation exposure and navigation-failure rates.
Feasibility & conclusion
X23D has market feasibility, but it is dependent on how it is marketed. The clinically significant breach rate (12%) is higher than competitors', a complete turn-off for surgeons aware of those competitors. The plan therefore targets very experienced surgeons in areas untouched by X23D's advanced competitors, converting them with the less-radiation and lower-cost message. A path to FDA approval exists via the substantially equivalent Zeta Surgical device, and AR / minimally invasive equipment is worth trialing to reduce clinically significant breaches.
In short, the report proves X23D has limited feasibility: it holds the market advantages of lower radiation and cost but lacks the advantage of surgical accuracy due to its higher clinically significant breach rate, a rate that would erase feasibility were it not offset by external factors and the right customer base. If the AI improves and that breach rate falls below competitors', X23D could dominate the AI-imaging market in spine. A technology feasibility report like this one would have prevented the recalls and patient deaths of the Medtronic Stealth portfolio.
References
- AdventHealth. (2025, March 28). Accelerating orthopedic innovation through research. AdventHealthMD.
- Ajibade, A., Onyeka, S., Cai, Z. R., Daneshjou, R., & Olatunji, T. (2024). A scoping review of reporting gaps in FDA-approved AI medical devices. NPJ Digital Medicine, 7(1), 273. https://doi.org/10.1038/s41746-024-01270-x
- Alexandrovsky, V., Stüer, C., Burger, R., et al. (2010). Clinical acceptance and accuracy assessment of spinal implants guided with SpineAssist surgical robot. Spine, 35(24), 2109–2115.
- AO. (2023). Fig 4 [Image]. AO Foundation.
- Asada, T., Subramanian, T., Simon, C. Z., et al. (2024). Level-specific comparison of 3D-navigated and robotic-arm-guided screw placement: an accuracy assessment of 1,210 pedicle screws in lumbar surgery. The Spine Journal, 24(10), 1872–1880. https://doi.org/10.1016/j.spinee.2024.05.013
- Baumgart, L., Ille, S., Kirschke, J. S., Meyer, B., & Krieg, S. M. (2023). Radiation doses and accuracy of navigated pedicle-screw placement in cervical and thoracic spine surgery. Journal of Neurosurgery: Spine, 39(3), 363–369. https://doi.org/10.3171/2023.4.SPINE23174
- BrainLab. (2025). How spine navigation amplifies surgery [Image]; Spinal Planning [Image]. BrainLab.
- CBYON Eclipse. (2024). Software Features [Image]. MSS.
- Center for Devices and Radiological Health. (2023). StealthStation S8 application recalled due to a software glitch. U.S. Food & Drug Administration.
- Center for Devices and Radiological Health. (2025). Artificial intelligence and machine learning in software as a medical device. U.S. FDA.
- Chiou, S. Y., Liu, L. S., Lee, C. W., et al. (2023). Augmented-reality surgical-navigation system integrated with deep learning. Bioengineering, 10(5), 617. https://doi.org/10.3390/bioengineering10050617
- Chong, X. L., Kumar, A., Yang, E. W. R., et al. (2020). Incidence of pedicle breach following open and minimally-invasive spinal instrumentation. BioMedicine, 10(2), 30–35. https://doi.org/10.37796/2211-8039.1016
- Clark, C. (2024, November 14). Surgeons billed $2 billion for unnecessary spine surgeries. MedPage Today.
- Deloitte. (2024, December 12). As generative AI asks for more power, data centers seek cleaner energy solutions. Deloitte Insights.
- Devito, D. P., Kaplan, L., Dietl, R., et al. (2010). Clinical results of robotic-guided spinal surgery. Spine.
- Eniko & Rein. (2014). Figure 4(c) [Image]. Journal of Medical Engineering. https://onlinelibrary.wiley.com/doi/10.1155/2014/976323
- Grand View Research. (2023). AI in medical-imaging market size and share report, 2030.
- Grabala, P., Helenius, I., Kowalski, P., et al. (2023). Figure 1 [Illustration]. Washington University School of Medicine.
- Hao, K. (2020, December 7). Training a single AI model can emit as much carbon as five cars in their lifetimes. MIT Technology Review.
- Hayashi, D., Roemer, F., Mian, A., et al. (2012). Fig 8 [Image]. American Journal of Roentgenology. https://www.ajronline.org/doi/10.2214/AJR.11.6497
- IJCRI. (2016). Cover figure [Image]. International Journal of Case Reports and Images.
- Jackson, I. (2017, May 3). FDA issues warning on Medtronic surgical-navigation tools after patient deaths. AboutLawsuits.com.
- Jassar, S., Adams, S. J., Zarzeczny, A., & Burbridge, B. E. (2022). The future of artificial intelligence in medicine: medical-legal considerations. Healthcare Management Forum, 35(3), 185–189. https://doi.org/10.1177/08404704221082069
- Jecklin, S., Jancik, C., Farshad, M., Fürnstahl, P., & Esfandiari, H. (2022). X23D, Intra-operative 3D lumbar-spine shape reconstruction based on sparse multi-view X-ray data. Journal of Imaging, 8(10), 271. https://doi.org/10.3390/jimaging8100271
- Lewandrowski, K. U., Soriano-Sánchez, J. A., Zhang, X., et al. (2020). Regional variations in acceptance and utilization of minimally-invasive spinal-surgery techniques among spine surgeons: results of a global survey. Journal of Spine Surgery, 6(Suppl 1), S260–S274. https://doi.org/10.21037/jss.2019.09.31
- Lopez, C. D., Boddapati, V., Lombardi, J. M., et al. (2020). Recent trends in Medicare utilization and reimbursement for lumbar-spine fusion and discectomy procedures. The Spine Journal, 20(10), 1586–1594. https://doi.org/10.1016/j.spinee.2020.05.558
- Luchmann, D., Jecklin, S., Cavalcanti, N. A., et al. (2024). Spinal navigation with AI-driven 3D-reconstruction of fluoroscopy images: an ex-vivo feasibility study. BMC Musculoskeletal Disorders, 25(1), 925. https://doi.org/10.1186/s12891-024-08052-2
- Medress, Z. A., Jin, M. C., Feng, A., et al. (2020). Medical malpractice in spine surgery: a review. Neurosurgical Focus, 49(5), E16. https://doi.org/10.3171/2020.8.FOCUS20602
- Muralidharan, V., Adewale, B. A., Huang, C. J., et al. (2024). A scoping review of reporting gaps in FDA-approved AI medical devices. NPJ Digital Medicine, 7(1), 273. https://doi.org/10.1038/s41746-024-01270-x
- NewYork-Presbyterian. (2022, September 14). Exercising due diligence with new technologies in spine surgery. Advances in Pediatric Orthopedics.
- OpenAI. (2025). X23D billboard mockup and X23D LinkedIn / insurance-conference ad mockup [Generative-AI images]. ChatGPT.
- Orthofix. (2025, March 27). Navigation.
- OUHSC. (2021, August 27). Collaboration leads to high-tech surgical-visualization devices at OU Health. InsideHSC.
- Public Health. (2025). Artificial intelligence in healthcare. European Union.
- Raad, M., Reidler, J. S., El Dafrawy, M. H., et al. (2019). U.S. regional variations in rates, outcomes, and costs of spinal arthrodesis for lumbar spinal stenosis in working adults aged 40–65 years. Journal of Neurosurgery: Spine, 30(1), 83–90. https://doi.org/10.3171/2018.5.SPINE18184
- Samdani, A. F., Ranade, A., Saldanha, V., & Yondorf, M. Z. (2010). Learning curve for placement of thoracic pedicle screws in the deformed spine. Neurosurgery, 66(2), 290–295. https://doi.org/10.1227/01.NEU.0000363853.62897.94
- Scorza, D., Hadji, S., Cortés, C., et al. (2020). Fig 5 [Illustration]. Medical Image Analysis.
- Segal, D. N., Grabel, Z. J., Shi, W. J., Gottschalk, M. B., & Boden, S. D. (2018). The impact of insurance coverage on access to orthopedic-spine care. Journal of Spine Surgery, 4(2), 260–263. https://doi.org/10.21037/jss.2018.05.22
- Stryker. (2025). SpineMap Go [Image]. Stryker NAV3i Platform.
- Taghva, A. (2025). Understanding the financial implications of minimally-invasive spine surgery. Alexander Taghva, MD Neurosurgery.
- World Health Organization. (2024). Enhancing radiation-safety culture in health care: guidance for health-care providers. WHO.
- X23D AG. (2025, January). Launch of joint Innosuisse project, collaboration between X23D AG and Universitätsklinik Balgrist [LinkedIn post].